13 Therefore set I in the lower places behind the wall, and on the higher places, I even set the people after their families with their swords, their spears, and their bows. 14 And I looked, and rose up, and said unto the nobles, and to the rulers, and to the rest of the people, Be not ye afraid of them: remember the Lord, which is great and terrible, and fight for your brethren, your sons, and your daughters, your wives, and your houses. 15 And it came to pass, when our enemies heard that it was known unto us, and God had brought their counsel to nought, that we returned all of us to the wall, every one unto his work. 16 And it came to pass from that time forth, that the half of my servants wrought in the work, and the other half of them held both the spears, the shields, and the bows, and the habergeons; and the rulers were behind all the house of Judah. 17 They which builded on the wall, and they that bare burdens, with those that laded, every one with one of his hands wrought in the work, and with the other hand held a weapon. (Nehemiah 4:13-17)
In the time of Nehemiah, the threat of attack was ever present, making it necessary to defend God’s people. The plan was simple – build the wall so the people could live in peace and safety. How would they do it? Families were responsible for repairing their own section of the wall (Neh. 3). While some worked, exposing themselves to danger, others stood guard. The enemy, seeing that “the breeches began to be stopped”, became “very wroth.” (Neh. 4:7) Nehemiah encouraged his people, saying, Be not ye afraid of them: remember the Lord, which is great and terrible, and fight for your brethren, your sons, and your daughters, your wives, and your houses. -Nehemiah 4:14 Eventually, the enemy gave up, …for they perceived that this work was wrought of our God. -Nehemiah 6:16
What does this have to do with vaccines? A lot. Remember herd immunity? That’s the principle whereby, most people in any given community get vaccinated, thus providing protection for the unvaccinated and the vulnerable (or immune-suppressed) from specific diseases by not allowing those diseases an opportunity to “catch on fire”. An infectious disease that finds its way into that community from the outside would quickly die out if it could not easily find another person to infect. On the other hand, if some were exposed and there was a lack of herd immunity, an infection would find that community defenseless, and many who were not immune would contract that disease.
Here an important point needs to be made – individual immunity against a specific disease has nothing whatsoever to do with a strong immune system, nor with diet, nor with cleanliness. Anyone who has a strong immune system, eats healthy, takes special supplements, and practices the best personal hygiene is still not necessarily immune to certain diseases. Diet, cleanliness, and overall health (including a person’s genetics and strength), ARE important in determining the susceptibility of a person to a disease, and the severity that they may get it – perhaps even if they will survive. But do not be confused – susceptibility and immunity are not interchangeable – having a strong immune system is not the same thing as having immunity. Any person’s body that is not immune (whether naturally, through past exposure, or through vaccines) will need to go through the process of fighting against any given disease that they are exposed to. It is through this process of the body fighting against the virus or bacteria, that antibodies are normally developed in that person. This (the antibodies) is what makes them immune. Thus, the only way an individual can be immune to a specific disease is for them to develop antibodies against that disease, either through a personal battle with that disease or through tricking the immune system into thinking it’s under a full-scale attack through the use of a vaccine (a killed or weakened form of that disease) and thereby stimulating the body to produce antibodies.
Herein rises the confusion about vaccine-induced health issues. The only way antibodies can develop in an individual’s body is through the process of fighting off the disease (or the perceived disease with vaccines). It is while the white blood cells are fighting off the disease that a fever or other physical complications will arise. This is NOT caused by the vaccine, per se, rather it is a natural result of the body fighting against the virus or bacteria of the disease they have just been exposed to through the vaccine, and therefore, it (the fever or any other similar physical malady) is a necessary part of the process of developing the required antibodies. (i.e. Any time white blood cells are dying off while fighting a disease, that person’s body will develop a fever or some other normal side effect as a natural result of that battle with that disease.) In rare instances, as you will see, this process of developing the antibodies can cause unintended complications.
Immunity is like the wall that surrounded Jerusalem. Nehemiah found the city wall in shambles, which is like a community which has no herd immunity. The most vulnerable (the children and the elderly), were defenseless and at the mercy of the enemy, if an attack were to come. Eventually, the walls (of immunity) of the city stood strong. This would have been accomplished by the community gaining herd immunity either through directly fighting the disease or through vaccinations. There would still be vulnerable people (the immune-compromised – such as chemo recipients, the very old, and the very young), but they would be able to stand in the middle of the city and be defended by the wall. Another example of “herd immunity” is a herd of strong musk oxen standing in a circle, shoulder to shoulder, facing the wolves, with their young protected in the center.
Where there were breeches in the wall, there was an opportunity for the enemy to gain entrance and wreak havoc on the weak who were inside. This is like non-immune individuals (often unvaccinated) seen as breeches standing in that wall, potentially allowing the enemy to enter. This is why those who unquestioningly advocate the use of vaccines ask, “Why don’t you (those who do not vaccinate) fight for your brethren, your sons, your daughters, your wives, and your houses (not to mention, your communities) – by getting vaccinated?!” It’s a fair question.
The Bible does not say how many builders were attacked, or how many died for the cause of building the wall. According to cold statisticians, any such loses would be considered isolated cases of “collateral damage” – casualties that were unfortunate yet necessary for the greater good of protecting the community. In the case of our analogy (of the wall of Jerusalem and the wall of immunity) those who were injured and killed while building the city wall, would be the same as those who were injured, or those who died, while building the wall of immunity (i.e. those killed or injured by vaccines).
It is here that our analogy breaks down, and where we can identify the chasm of discord between those who are unquestioningly either pro-vaccination or anti-vaccination. Surely, any godly man in Nehemiah’s day would have risked his life building that wall to protect his family and his community. But that’s the catch, to keep the analogy true – it is not the men who must build the wall of herd immunity, it is the children! Yes, the parents may be like those standing guard over the workers (by providing good nutrition, medicine, and access to good healthcare), but it is the workers (the children receiving the vaccines) who are exposed to the attacks and placed in the line of danger (vaccines). While godly parents would gladly take ALL the risk of being both guard and builder, our analogy will allow ONLY the children to be exposed to the risk. This is why so many parents are unquestioningly anti-vaccine. Not anti-vaccine out of a sense of neglect to protect the community, but anti-vaccine out of a sense of need to protect their children.
It would make little sense to accept a high risk to the workers (our children) through vaccines that are potentially dangerous, for a disease that has a low risk of long-term problems. Likewise, it would bring clarity to the confusion if it was clear that the risk to the worker was low (with a “safe” vaccine), and if it was clear that the disease was almost universally deadly. So where do we go from here to get more information to help us decide if vaccines are worth the risk?
Here is one last concept to consider before I answer that question. Many modern epidemics have started in plain communities, because the “Herd Immunity” was weak. The largest outbreak of measles in the U.S. that occurred in decades started when a missionary from a plain church brought back a case of the measles from the Philippines in 2014. Hundreds were affected (382 cases), some with permanent complications, however, none died (even though there are still cases of deaths in the U.S. due to measles).i Normally, there have been an average of about 63 cases per year.ii The last case of a wild strain of polio in the U.S. was in an Amish community in 1979, which left 10 people paralyzed. In 1991, the last large rubella outbreak (across six states) resulted in hundreds being infected. Of those, 89 Amish and Mennonite women contracted the disease while they were in their first trimester of pregnancy. Ten children (possibly 7 more) were born with multiple serious birth defects associated with Congenital Rubella Syndrome.iii There are normally less than 10 cases of Rubella annually, with an average of less than 1 case of CRS per year – for the entire country.iv I mention these cases only to point out that there is a vulnerability that may not be recognized in a community of less than one million plain people that is relatively small in size when compared to a population of 325 million in the entire U.S. Certainly, there are other outbreaks not associated with the plain communities, such as in colleges and other schools, because vaccines do not produce 100% immunity, and sometimes the immunity wanes over time.
VAERS
So how do we know more about the risks of vaccines? There is a national “Vaccine Adverse Event Reporting System” started in 1990. Here (vaers.hhs.gov) any person can access information concerning adverse effects of vaccines. Healthcare workers are required to report adverse reactions to vaccines, however, ANYONE (even parents) can voluntarily file a report. Its main purpose is to monitor vaccine safety. For example, if there is a batch of vaccines improperly or unsafely manufactured, and a cluster of complications occurs, such a reporting system would aid in discovering and isolating the problem quickly and accurately. Likewise, it can be used for monitoring adverse reaction “trends” due to the nature of the vaccines. VAERS is co-managed by both the Centers for Disease Control and Prevention (CDC) and the U.S. Food and Drug Administration (FDA), thus providing multiple forms of oversight so it is not so easily influenced by corporate dollars and special interests. Finally, VAERS is open to the public, so you do not need to be a professional to access the data, you can see it for yourself.
One study showed that from 1990-1993, there were 54 million doses of the oral polio vaccine given. The oral polio vaccine uses a weakened virus, but is easy to give, since it is mixed with sugar water and easily given to the child by mouth. It is very effective, but in rare cases it can CAUSE polio. Over those 3 years, there were seven cases of vaccine-caused polio, making the risk of getting polio from the vaccine about one, in eight million.v Because the last case of natural (as opposed to vaccine-caused) polio in the United States was in 1979, this average of two cases of polio per year was considered too high. So, because of the recognition of these numbers, the vaccine was switched to the injectable form, since it is a dead virus, and thus cannot cause polio.
Why vaccinate at all? The idea is to eradicate polio (throughout the world), in the same way that smallpox was finally eradicated, (with the last case being in 1977). The World Health Organization estimates that there has been a 99% reduction in the cases of polio, from the beginning of its worldwide eradication program that started in 1988, with 350,000 cases in that year, to just 22 cases in 2017. They estimate that 16 million people have been spared from contracting polio-paralysis during this time due to this effort. If there is even one infected individual, there is still the potential for it to rekindle a bonfire that can spread across continents, until the last case is smothered out by herd immunity.
Still, there is a cost. If you’re one of the 16 million who never got polio but would have gotten it had it not been for the vaccines, chances are that you will not have a full appreciation of what you were spared from, especially if you are one or two generations removed from the time when polio was commonplace. Yet, if you are one of the average of two children per year in the U.S. who got the vaccine-associated polio, you would certainly be reminded of that fact every time your friends went out to run and play. (While the oral polio vaccine is no longer used in America, it is still widely used in the developing nations, due to its ease of use and its acceptability. Therefore, vaccine-associated polio in America is now practically nil.)
The fact is that for many, but (not all) childhood vaccines, you are primarily vaccinating to protect the community, not your individual child. This may also be one reason why numerous plain people look at the medical community with some suspicion. There is an expectation that a doctor is always an advocate of the individual patient. However, regarding the issue of vaccines, they are the advocate of the community first, then of their own patient second. In the vast majority of cases, there is no conflict, but when complications occur, patients and their families will rightly ask, “Was this avoidable?”
Many people believe there are more complications than “only” catching the disease, bad as that might be. This is true. Frequently there are minor complications (for example, a fever and a rash), that do not cause long-term problems. These are not unexpected in a body’s immune system that is “gaining experience” in fighting a mini-battle against the target organism. This is how immunity works; that way if the body “sees” it again (by being exposed to someone that is sick with the actual, culprit organism), the person’s body will immediately recognize it and defeat it before it gains a foothold. Then there are complications that are very scary to both parent and child, but are most often only time-limited, and don’t recur, such as febrile seizures. Finally, there are the complications that cause permanent disability and death. This is where we will now focus our attention.
The table below shows us the VAERS data for each organism over the last 10 years, and the complications for each. For simplicity, I will only address childhood vaccines covering children up to the age of 18 months. Some of you have questions concerning things like mercury, aluminum, and other potential causes of reactions. Here I will not go into every possible cause – that will need to wait for another time. This is because the statistics listed cover ALL causes, hypothetical and real alike, yet the numbers all remain the same. I will caution however, to not draw the wrong conclusions ahead of time, since as we will see, you can’t believe everything you read (or see).
Table 1
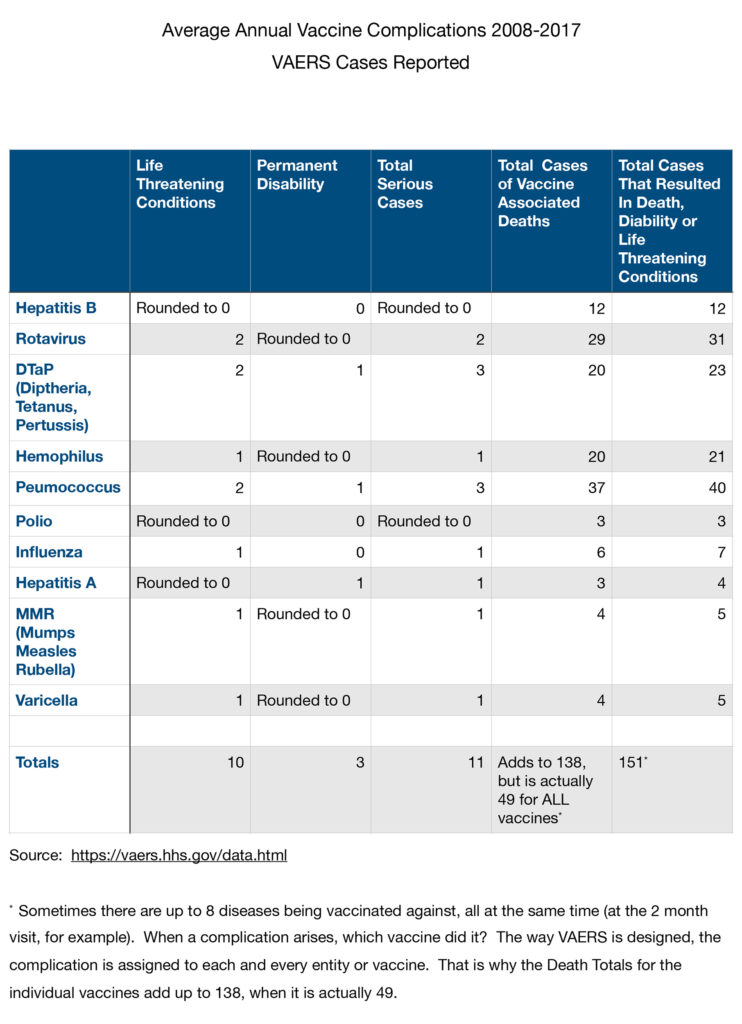
Notice that some vaccines are “better” (or less bad) than others. Why is that? I put the vaccines in a certain order. They are not in alphabetical order, rather they are in the order that a child would receive them. Hepatitis B is given at birth, and the Hepatitis A, Varicella (Chicken Pox), and MMR (Mumps, Measles and Rubella) vaccines are first given at 12-15 months. Notice how the first vaccines (like the DTP) tend to be more “lethal”? There are a couple of reasons for this.
First, it seems to be a vaccine that tends to have more complications, mostly minor, such as fever or a rash. For this reason, it was reformulated to a DTaP in which the “a” stands for “acellular,” meaning that it was a more purified product. Second, and probably most importantly, the COD (Cause of Death) was most commonly due to SIDS (Sudden Infant Death Syndrome). SIDS is a condition where the baby goes to sleep and does not wake up. It most commonly happens in the first half year after birth – just when the “most dangerous” vaccines are given. For us in the medical field, it has been a perplexing issue, as we have not been able to isolate the exact cause. The best we can say is that it usually is associated with parents who smoke, the sleeping position (lying on the belly) of the baby, and big, deep fluffy blankets.
There are up to six doctor’s visits and six sets of vaccines that are recommended in the first 18 months (78 weeks) of a baby’s life. If a child has a reaction to a vaccine, it will generally occur within the first week of receiving it. Therefore, there are only six weeks out of the first year and a half, (for a child who is receiving the full course of vaccines), that are within 1 week of receiving a vaccine. If SIDS occurs randomly, there should be about 6/78ths (or about 8%) of SIDS deaths occurring within one week of receiving vaccines. If it is more than 8%, then yes, the vaccines are VERY suspect. If it is 8% or less, then any SIDS deaths that occur within one week of receiving vaccines are no more than what would be expected to have occurred randomly (though no less tragically).
So, what are the numbers? SIDS rates actually have been reduced by more than half, over the last 20 years, simply by placing the baby on his or her back to sleep. Still, in 2016, there were about 2,700 cases of SIDS, or an unknown reason for death. So, 8% of this number is about 216 cases of SIDS that would be expected if SIDS were to happen randomly, and not associated with vaccines. As it turns out, over the last 10 years, there have been an average of only 49 deaths (not 216 as expected) each year from ALL vaccines combined, for children up to 2 years old. Does this mean that vaccines protect against SIDS? Probably not, but it does mean that vaccines are less likely to be the cause for an extraordinary number of deaths. (Remember, VAERS is designed for the early detection of adverse effects, not for finely accurate statistics.)
Yet deaths do happen, and life-threatening conditions and permanent disabilities do come about because of vaccines. Nobody can deny this, but what is the alternative? The VAERS system reports an average of 11 cases per year of vaccine-associated, life-threatening conditions and permanent disability from ALL childhood vaccines. This includes anaphylaxis (airways closing off), brain infections, bowel obstructions, and just about anything else bad that could happen. Personally, I believe the actual number may be significantly higher than this. To be on the safe side, let’s assume this number is WAY under-reported, by a factor of 10. If this is the case, (and it may well be), there would be 110 serious, but not death-causing, cases annually. Complications that are serious tend to have “reporting sensitivities” that are close to the actual number, while minor complications are very under-reported. Thus, our estimate it likely an over-correction, but it will help to give clarity, as you’ll soon see.
When I first became a Christian, I needed to answer doubts I had about the doctrine of non-resistance. What clinched it for me was when one of my fellow aircrew members (a Christian), while trying to dissuade me, asked who would fight the wars if soldiers, sailors, and airmen all became Christians and decided not to fight. No sooner had the question left his mouth than the answer seemed quite clear – if nobody fought, there would be no need of wars. Of course, we are all born with the sin of Adam, so that is not likely to happen. But the point is that Christians make the world a better place for all, if they stick to their sound doctrinal convictions, no matter the cost.
Is it then unfair to ask ourselves the question, “What would happen if we all forsook vaccines? Would we, as our brothers’ keepers, leave the world, (of which we are the stewards), a better place?” Naturally, these are personal thoughts and positions, not approaching that of doctrine, but in 2014, the Centers for Disease Control (CDC) took it upon themselves to answer that very question. Their findings are shown in Table 2, where it is claimed that the number of American people saved by vaccines since 1964 is 731,700. Note that the numbers in the table are in the thousands of cases.vi
Table 2

However, the numbers in Table 2 assume 1960s treatments and technology. Plus, some diseases, such as diphtheria, could be managed much easier with today’s medicines and technologies. Diphtheria is caused by a bacterium that infects the throat, giving it a “Bull Neck” appearance. The airway can close as a gray membrane closes it off. This membrane cannot readily be scraped off since it bleeds easily. Another complication is that toxins which are produced can lead to paralysis and heart failure. Many years ago, anxious parents exposed their children to turpentine and tar fumes in a desperate, yet futile effort to cause them to cough up the membrane. Medically, it was initially treated with antitoxins, developed at the beginning of the 20th century. (Remember the children’s book about Balto, the sled dog, that ran antitoxin to save the children of Nome, Alaska?) Before the antitoxin, death rates for diphtheria were about 50%. Afterwards, rates were still as high as 20% in children under five years-of-age, and in adults over 40, but 5-10% for the rest – even with the use of antitoxin and antibiotics.vii This vaccine, introduced on a large scale in the 1930s, took a high of 200,000 cases per year in the 1920s, down to 2 cases per year over the last 14 years (in the U.S.). However, the World Health Organization (WHO) reports that there are still tens of thousands of cases per year (worldwide), and thousands of deaths. We know the numbers didn’t decrease mainly due to good sanitation and nutrition, because the rate of disease has diminished greatly in areas of the world that are still in extreme poverty yet have used vaccines.
Deaths due to measles also decreased worldwide from about 546,800 in the year 2000 to 114,900 in 2014, largely due to an MMR initiative by the World Health Organization. It (WHO) claims 17.1 million lives were saved during that time. (The accountants among you will note that this number does not come close to matching the data. It’s probably more like 3-4 million unless they are correcting for vast underreporting due to poor reporting sensitivity, which they don’t mention.)viii Yet big numbers of sick and dying children are real. When I did medical mission work in Africa, I witnessed a country in which one out of five children died before they were five years old – mostly from these very preventable childhood diseases.
But the problem I have with the estimates in Table 2 is that realistically, with modern technology, (while it is best not to get the disease in the first place), medicines and supportive measures would most certainly reduce the mortality rate to much less than the 10% they estimate. In 1995, in the wake of the Soviet Union collapse the Kyrgyz Republic faced an epidemic of diphtheria; but even with their strained resources, they saw only a 2.8% mortality rate, which is close to a quarter of the CDC estimate.iv So even if the numbers of these cases are exaggerated, those spared in America by vaccines are still in the hundreds of thousands.
Which brings me to this point, I believe some people are suspicious of government statistics and medical agents (doctors pushing vaccines) because of somewhat exaggerated statistics (though 2.8% of five million avoided-diphtheria cases is still a big number). In science, when trying to convince a skeptical crowd, speakers use conservative numbers. When speaking to a receptive crowd, or if the speaker thinks the audience isn’t smart enough to figure it out, he will use inflated numbers to make the case more impressive. There is too much bullying by those in the medical community – too much trying to convince parents that their child will be stricken with all sorts of diseases if they don’t get vaccinated.
This may be true for some vaccines, but let’s remember, most childhood vaccines are given to protect the community, not the individual child. Most unvaccinated people will be protected by herd immunity (if there are enough immune people in their home community), unless they or one of their acquaintances travel to areas of the world (as missionaries sometimes do) where the disease is still common. I believe that parents will make wise decisions, when faced with realistic data, and considering their family situations.
There is a chart available for download on the CDC website that provides a wealth of information, but it is too big to put in this article. This is the link: https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/appdx-full-e.pdf where it is available. I will draw from this chart to develop some points for comparison. For clarity, let’s look at those diseases for which there is still no medical cure once contracted. Let’s look at just ONE serious complication (encephalitis) from just ONE disease (measles). The chart says that vaccines prevented about 71 million (look closely, it’s not 70,748) cases of measles over 20 years (or about 3.5 million cases per year). The rate of encephalitis (a brain infection due to measles) is 1 in 1,000 cases, so there would be about 3,500 anticipated cases of encephalitis annually (with permanent disability or death) if there were NO vaccine (or herd immunity). Of these 3,500 people with encephalitis, 80% (or 2,800) will not make it (they will die!), and the remainder (700) will be severely disabled.
Let’s compare:
Present Conditions – With Vaccines
- 49 – Deaths per year, due to ALL childhood vaccines (as reported by VAERS)
- 110 – Average yearly cases of ALL permanent disabilities & life-threatening conditions DUE to ALL vaccines
Estimated Conditions – Without Vaccines
- 700 – Average yearly cases of ONE Complication (encephalitis) from ONE Disease (measles) if there were no vaccinations
- 2,900 – Deaths per year, due to measles alone if there were no vaccinations
- 600 – Average yearly cases of congenital rubella (babies with birth defects) if there were no vaccinations
- 62,200 – Average yearly cases of polio if there were no vaccinations
That’s a lot of numbers. You can draw your own conclusions as well as I can. Someday, scientists should be able to take a person’s own immature stem cells by a simple blood draw, and program (or “school”) them to produce antibodies for any number of diseases. It seems like there is a greater acceptance among plain people regarding stem cells (especially if they are their own). The vaccine issue will then become obsolete, because the side effects, minor and major, will be greatly diminished, if existent at all, while offering greater protection for both the individual AND society. Until then, we have the opportunity, Lord willing, to eradicate other diseases (next is polio, where two out of the three wild polio strains are gone forever – only Type 1 remains).
So, in the jumble of all these numbers, it is important to remember that there are real human lives at stake. We need to recognize the pain experienced by families in which a child is afflicted with a permanent disability, even death, due to a vaccine given to him or her. (This is no different from a situation in which a parent gives a medicine to his child, and the child undergoes anaphylaxis, and is severely injured or dies. In these situations, God recognizes the heart – the intent to do good.) At the same time, we also need to acknowledge that parents from developing countries mourn no less for their children than we do for ours, that we are our brother’s keeper, and that we do not live on an island.
In days of old, people used another term for “complication,” when stricken with illness, disability, or death. The term they used was “the hand of God.” For no matter how good or bad our science is, or no matter what decisions we think we make independently, He alone is sovereign. May God grant each of us wisdom as we consider His will in these matters.
In the next issue, I will discuss ways in which Christians have approached this difficult issue of vaccinations within their families and churches. We will discuss the rights the government has afforded us, and the trends in the future. I welcome your input and suggestions.
Endnotes:
- https://www.smithsonianmag.com/smart-news/ohio-measles-outbreak-wasnt-caused-anti-vaxxers-amishtraveler-180954090/
- https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6204a1.htm
- https://www.cdc.gov/mmwr/preview/mmwrhtml/00017145.htm
- https://wwwnc.cdc.gov/eid/article/24/4/17-1540_article
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1615747/?page=1
- https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6316a4.htm
- https://www.cdc.gov/diphtheria/clinicians.html
- http://www.who.int/news-room/detail/12-11-2015-measles-vaccination-has-saved-an-estimated-17-1-million-livessince-2000
- https://www.uptodate.com/contents/clinical-manifestations-diagnosis-and-treatment-of-diphtheria/abstract/3
Editor’s Note:
There seems to be some question by a few of our readers asking why we have been printing articles on this vaccine issue. Originally our burden was to publish the concern that many vaccines are grown on tissue from aborted fetuses. This fact is referred to by some as “tainted vaccines” and in our minds develops cause for concern when evaluating this in view of Christian ethics. This is the reason we decided to publish several articles on the matter.
However, in order to have a proper balance and perspective on the matter, we saw the need to first establish the historical facts of why, where, and how vaccines first came into use. It also seemed necessary to show the medical and scientific reason that the concept of vaccines is imperative to the health of human beings, by eradicating diseases that had become epidemic due to a lack of proper treatment options.
From the beginning we had planned to only print three (3) articles: 1) the introduction, origin, and the ongoing need, 2) the “tainted vaccine” issue, and then 3) a conclusion on various options with recommendations for us as Christians living in a fallen world. Due to questions and concerns that were raised by some, we saw the need to print several more articles to help bring clarity to the issue. The bottom-line is that some wanted to place us in the camp of the unquestioningly PRO-vaccination camp and others thought we were in the unquestioningly ANTI-vaccination camp, depending who it was and which article they were reading. The truth is that we were not trying to promote either camp, rather share the pros and cons along with some recommendations, then leave it up to individual families and churches to decide what is right for them.
We encourage each one to do their own research on the information listed in this article using the links that are supplied. Finally, lest it is thought that this is a non-issue or an outdated one, it may help bring some reality and perspective to the matter to start following the current epidemic of measles in Europe. In the first half of 2018 alone, there were already over 41,000 cases of measles documented and at least 40 deaths to date this year. This is directly linked to a strong push in their society over the last number of years by those who are anti-vaccine, therefore, many of their population are not immune and the herd immunity in their communities is diminishing. This is not one or two sources trying to create fear-mongering. See for yourself all the news sources who have reported on this current problem – “Europe is in the midst of a massive measles outbreak… The deadly virus has spread to 21 out of 30 countries in the region, and the World Health Organization says cases have hit a record high, with more than Europe’s annual total during the past five years. Italy has recorded more than 2,000 cases of the deadly infectious disease this year — and it’s one of seven European countries with more than 1,000 cases. (The others are France, Georgia, Greece, Russia, Serbia, and Ukraine.) England’s National Health Service just announced that its ongoing outbreak involves 876 cases — more than three times the 2017 amount.”i
One source stated, “Immunity rates in parts of Europe are lower than in some African countries.”ii Another source wrote, “Most cases in England are being seen in teenagers and young adults, the group born at the turn of the millennium when anti-vaccination fears exploded into the mainstream after now-retracted paper from disgraced physician Andrew Wakefield claimed it causes autism.”iii While still another source had this to say, “Over 41,000 cases of measles have appeared in Europe this year, and the trend may spread to the U.S. if the anti-vaxxer community continues to grow… Forty have died from the European measles outbreak, a disease spread that was unthinkable less than a decade ago… Experts claim European countries hold higher populations of anti-vaxxers, adults who chose not to vaccinate their children for the main, preventable diseases… It’s the main factor leading to the outbreaks… It’s unacceptable to have in the 21st-century diseases that should have been and could have been eradicated.”iv
These statements are the conclusions of the various health agencies who are desperately trying to reverse the problem. Are these logical conclusions? What would you do about a mass medical situation of this nature? Would you feel comfortable if your neighbor would travel over to one of these hotspots in Europe right now, then come back and invite you and your young children over for a Friday evening cookout next week? Christ taught that we are to love our neighbor as ourselves. So, how do we make that practical? We’ll consider more about that in the next issue.
Endnotes:
- https://www.vox.com/2018/9/20/17875238/measles-cases-europe-record-high-austerity
- https://www.economist.com/europe/2018/08/25/anti-vax-fears-drive-a-measles-outbreak-in-europe
- https://www.independent.co.uk/news/health/measles-epidemic-europe-record-high-symptoms-vaccines-who-world-health-organisation-a8499491.html
- https://www.vox.com/2018/9/20/17875238/measles-cases-europe-record-high-austerity
More Links
- https://www.cnn.com/2018/08/20/health/measles-europe-record-who-intl/index.html
- https://www.newsweek.com/measles-outbreak-europe-warns-us-anti-vaxxers-possibilities-experts-say-1180192
- https://www.bbc.com/news/health-45246049
- https://www.nbcnews.com/health/kids-health/measles-outbreak-raging-europe-could-be-brought-u-s-doctors-n922146

0 Comments